
19 weeks into our third pregnancy, our daughter was diagnosed with transposition of the great arteries. What would it mean?
Inside Out
On the lunarscape of an ultrasound display, my daughter’s heart looks like:
- the cross-section of a walnut
- a narrow waterfall
- the number 8
- the mouth of a guppy, opening and closing
- In the novel Gossip Girl, a photograph taken of some unnamed part of Serena Van Der Woodsen causes quite a stir. My daughter’s heart looks like how I’d imagined that photograph would.
One of the great, enjoyable mysteries of any pregnancy is what the baby will look like. How strange, then, to know my daughter’s interior so intimately months before I saw her face.
A few years ago, an artist friend of mine did a series of sculptures on our interiors. Women’s insides — you could tell they were women’s, somehow, even without the identifying parts — sloping and slumping and looping and proudly sagging in ways forbidden to our exteriors. Taking them in (and doing my best not to reach out and touch (they were very tactile, these interiors)), I was struck by how little I, and presumably most of us know our own guts from anyone else’s. Where the exterior is personal, constantly scrutinized; the interior is anonymous.
Over 3.7 million babies will be born in the US in 2021. At birth — or, rather, on all the ultrasounds leading up to and immediately after her birth, my daughter’s heart looked markedly different from all but about 1,000 of them. Twenty three weeks ago, I couldn’t have told you that. Twenty three weeks ago, if asked to draw a heart, I’d have given the Valentine’s version.
I can now draw a heart — both the normal kind and my daughter’s variation — about as well as someone with remarkably poor fine motor skills can.
Head-on, a normal heart looks like:
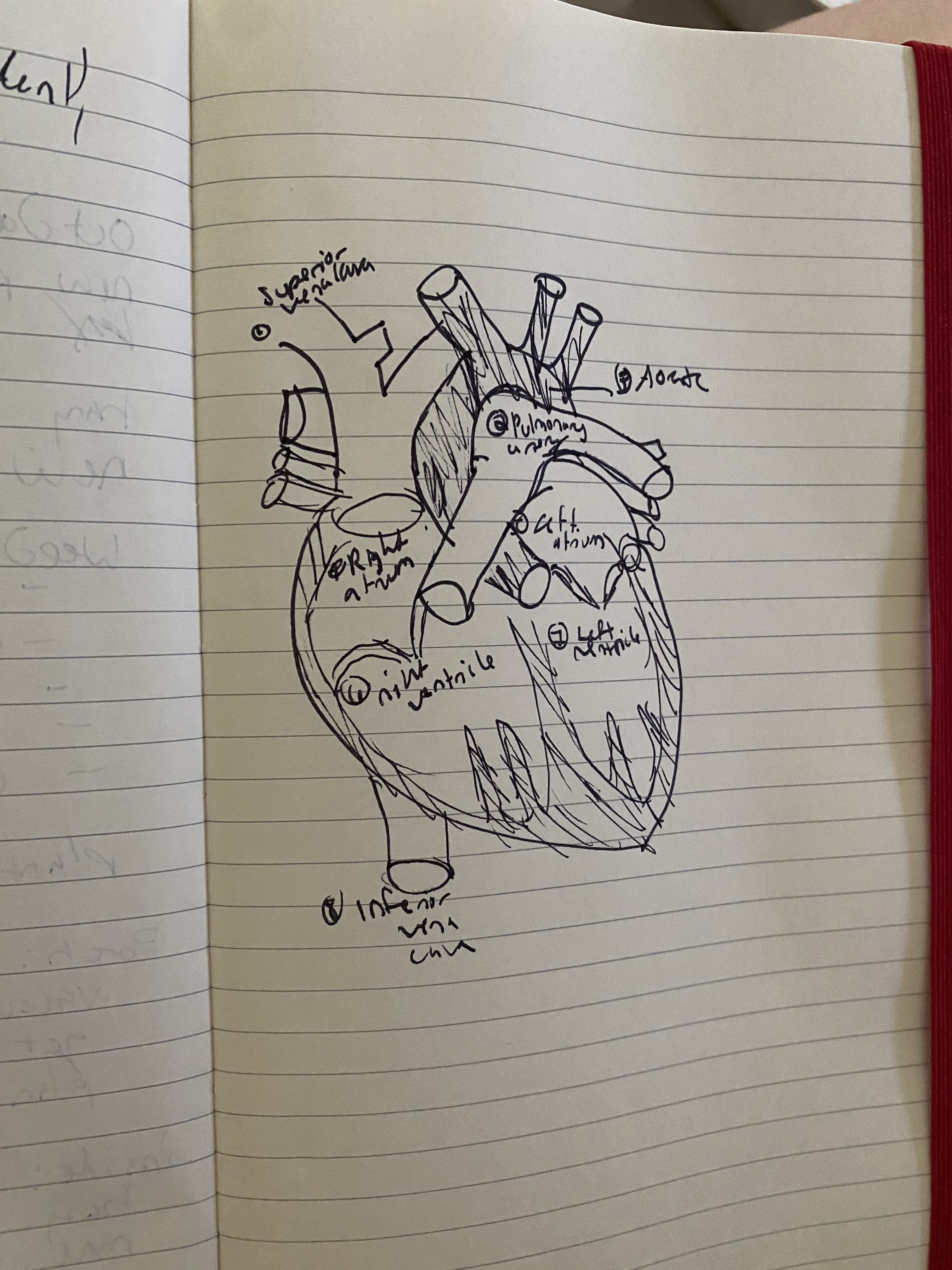
While my daughter’s looks like:

Can you spot the differences?
A brief cardiac anatomy lesson from an unqualified author
The heart’s purpose, in a nutshell, is to pump blood to the rest of the body. Because the body is, more or less, a hematologically closed system, the blood it makes use of is recycled — and the heart manages the recycling process. It takes the already-circulated, oxygen-poor blood and enriching it with new oxygen it gets from the lungs before sending it back out.
The parts of the heart that are most critical to this ingress-enrich-egress situation are the right and left ventricles (these look, in this head-on view, like fat jalapeno peppers), and the two large arteries, the pulmonary and the aorta. The right side of the heart manages ingress; the left, egress. Illustrations of the heart tend to use color to denote these separate functions: blue for the incoming and red for the outgoing blood.
My daughter was born with a congenital heart defect called transposition of the great arteries, or TGA. In the illustrations of her heart, the deep blue of the right atria and ventricle turn a muted sort of purple, and the pulmonary artery and aorta, normally entwined, stand aloof, in parallel. This is because the pulmonary artery, which is supposed to connect to the right ventricle, and the aorta, which is supposed to connect to the left, have transposed. In effect, you’ve taken a crazy eight and broken it into two separate loops.
On its face, this transposition renders the heart useless, eternally sending the same oxygen poor blood back to the body and the already oxgenated blood back to the lungs.
In blunter terms: the body cannot survive on a transposed heart.
And yet: the fetus, this inchoate, initially nearly brainless thing, finds a way to get some reoxygenated blood back into the circulatory system. Often, as in my daughter’s case, it finds several ways.
Every fetal heart has one point where the pulmonary artery and aorta connect directly, a little vessel called the patent ductus arteriosis. In a normal heart, this ductus serves no purpose, and, left alone, will close off within days of birth. In a transposed heart, this small connection point allows for some mixing of blood.
Many transposed hearts also fashion their own, additional mixing points, whittling little holes between the atria (atrial septal defects) or the ventricles (ventrical septal defects). The implication of agency here is wrong, and yet. These so-called defects, to a transposed heart, are critical assets. My daughter, who had both an ASD and a VSD, was born pink, and maintained such adequate levels of oxygen saturation that her surgery was delayed, twice. But I’m getting ahead of myself.
“We’re shadowed. But we’re fighting the shadow.”
My husband and I got our first clue that there might be something wrong with our daughter’s heart at the anatomy scan. We had just learned that the baby we’d been sure would be a third boy was, in fact, a girl, and were basking in this unexpected reversal when it occurred to me that the ultrasound tech was spending a lot of time trying to zero in on a specific angle of the heart. I say trying, because, for a good while, she wasn’t taking any photos, and when she did take one, she didn’t move on. The doctor would take another look, she said. Maybe he’d catch her in a better position.
The doctor, a kindly man in his mid-fifties, did not catch her in a better position, because there was no better position, though he didn’t say this. Instead, he said that he saw much to encourage him — the four chambers of the heart were well-formed, the brain looked great, the baby was moving like mad — but that he and the tech were having a hard time getting a view of the right outflow tract. He would send us to Boston Children’s Hospital to get an echocardiogram — a much more detailed ultrasound of the heart. “Fifty percent of the time, we just aren’t able to see what we need to with a regular ultrasound,” he said.
Thus began a period in which I paid very close attention to odds. A period in which a 5%, a 2%, even a 1% chance became an odd I didn’t like, though that initial 50 would be the largest (or smallest) we’d get.
After the 2016 election, the election modeler Nate Silver got hauled onto a lot of carpets, and it was his defense that I kept thinking of during this period. Which was: a 3 in 10 chance of winning is not a 0 in 10 chance. The model was not wrong, it was only that the less likely — but still very much possible — scenario had won out.
The odds of our daughter having TGA were 3000:1. Who would take that bet? And yet, the 1 had won, if you can call it winning.
This was also a period in time wherein I learned what the heart was supposed to do, and the many ways it might not do what it was supposed to do, and the names for the parts involved. Some of those names, like, say, “right outflow tract,” are rarely, if ever used outside of the medical profession. Which means that if you google them, the results are all research papers and ultrasound diagnostic instructions [1].
I struggled through as many of the more recent ones on TGA — particularly on longer-term outcomes of children born with TGA, and on ways to influence those outcomes — as I could find. This sort of research is common to any parent of a child with a less-common condition, but getting anything useful from it takes time, patience, and a basic familiarity with statistics, study methodologies, and the condition itself.
In my case, this self-driven research was not necessary. TGA is rare but not extremely rare; at Boston Children’s, it is somewhat common (our cardiologist estimated that the hospital performs 1-3 surgeries to correct it each week). I learned nothing in those papers that wasn’t much better explained by our daughter’s cardiac team, but then again, I had access to “Long-term outcomes of the arterial switch operation for transposition of the great arteries and ventricular septal defect and/or aortic arch obstruction” and “Neuropsychological and Psychiatric Outcomes in Dextro-Transposition of the Great Arteries across the Lifespan: A State-of-the-Art Review” 24/7; reading them made me feel, in some small way, like I was doing something.

I’d guess that at this point, twenty four weeks post-diagnosis, someone has drawn me a transposed heart at least ten times. Most of the drawings were black and white, marker on a whiteboard or ink on paper, though the NP at the NICU used colored pencil, blue and red, for the blood.
The first heart sketch was drawn by our unborn daughter’s newly appointed cardiologist in a small conference room off one of the passageways connecting Boston Children’s to Brigham & Women’s. Black marker on a whiteboard. I watched it take shape in a dazed sort of way, occasionally nodding, feeling hapless to be before a whiteboard without my notebook. The echocardiogram confirming that my doctor and ultrasound tech had been right to send us here had wrapped up minutes earlier, with the arrival of the cardiologist. “There’s an issue with your daughter’s heart, but it’s completely fixable,” he’d said, before leading us to the conference room. I had not thought of hospitals as places requiring conference rooms, nor any of the other standard trappings of office work; it occurred to me then that this was the first conference room I’d been in since March of 2020.
The heart sketch is the starting point for the condition’s explanation. No one ever asked if I was a visual learner (I am not) before the drawing commenced. I looked at each sketch without seeing it, and — after that first whiteboard session — took notes on what was said. Certain expressions appealed to me, such as comparing the operation to fix the transposition to “switching jumper cables,” or explaining the process of moving the coronary arteries to cutting out and reattaching the button as well as its thread.
Order of explanations accompanying the heart sketch:
- The normal heart
- The issue and its fixability, in abstract. (That we had only a half a second of awareness of the issue (or rather, confirmation) before we learned of its solvability was a supreme kindness, or a case study in not burying the lede.)
- The issue in specific (aided by the heart sketch).
- The fix.
The fix
The fix, which is called an Arterial Switch Operation, is ingenious in its simplicity. Cut the pulmonary artery and aorta above the valves, and switch them, so that the pulmonary is going into the right ventricle and the aorta, into the left. Doing this requires the surgeon move the right and left coronary arteries off the pulmonary artery, then switch the great arteries, and then reattach the coronary arteries to the aorta. It’s this bit, the surgeon would tell us, that is the trickiest, as an infant’s coronary arteries are tiny — the width of sewing thread.
For all that it is done on <7 day old infants, the ASO is astoundingly successful, with an average survival rate of +98%. In the majority of cases, it is the only corrective surgery the patient will need.
The ASO was pioneered by a Brazilian cardiac surgeon in 1975, though it didn’t become the standard procedure for fixing TGA until the 90s. Before the ASO, TGA patients underwent a more complicated — and less effective — procedure called the Atrial Switch Operation, aka the Mustard/Senning procedures. Before this, they mostly died [2]. As I told my father, there has never been a better time to be born with TGA.
Luck and the importance of prenatal diagnosis
I spent a fair amount of time in those early post-diagnosis weeks thinking: at least it’s not [x | y | z]. But then I started to spend a lot of time in the hospital lobby and elevators and halls and various ICUs, and invariably I’d see a child with [x | y | z] — and more so, I’d see their parents. There is no comfort to be gained from the game of at-least-it’s-nots.
Which is not to say we were not extraordinarily lucky. First, that, as I mentioned, our daughter would be born in 2021, and not 1980. Second, that we happened to live forty minutes from one of the best pediatric cardiology hospitals in the world. Third, that we had family members available to help watch our other children while we were in the hospital. Fourth, that we had good health insurance. (We are going to need it.) And last, and most importantly, that the diagnosis was prenatal.
TGA is the most commonly missed prenatal diagnosis of any CHD — currently, less than half of all cases are diagnosed prenatally. This is important, because prenatal diagnosis improves post-natal outcomes — in fact, it’s the only prenatal intervention that does. With a prenatal diagnosis, the parents and pediatric cardiac team can start planning for post-natal care right away, including making sure that delivery takes place in a hospital with a NICU. Most critically, members of this team will be in the delivery room and will assess the baby immediately after birth to determine whether any immediate interventions are needed. In addition to being extremely helpful for the baby, prenatal diagnosis also saves parents from what I can only imagine would be an extremely scary post-delivery experience (TGA babies are often born blue, or become so over the first few days of life) (not to mention a whole lot of last-minute logistical scrambling). So, if you are expecting and reading this, please, make sure your ultrasound tech and radiologist look for the TGA markers during the anatomy scan. In general, make sure they spend a good while on the heart. Healthcare providers who have had proper CHD screening training will catch up to 95% of simple CHDs and 90% of complex CHDs with an ultrasound, and the CDC and AHA are working to increase access to this.
The above isn’t meant to be alarmist — after all, the overwhelming odds are in favor of the markers’ absence. But… just … check that box off, will you? (And if you aren’t sure your current provider is trained to give a thorough CHD screening, please, try to get one at the nearest place that can.)
Laissez les tempes foux rouler (what it was like)

One of my reasons for writing … whatever this is was to give expecting parents who have received a prenatal diagnosis an account of what the birth, pre-surgery, surgery, and post-surgery experience for the parents of a transposition baby was like. This was something I myself very much wanted and could not find online (the patient stories available on some hospital sites are better than nothing, but short on detail and heavy on marketing plugs).
Caveat lector: n=1. But one is (I hope) better than 0.
At the point of diagnosis, our cardiologist told us to expect a hospital stay of about a month. In the end, we were there for fifteen days. The timeline looked like this:
- 7/21/21: give birth (induced around 4am, and our daughter was born 12 hours later)
- 7/21 – 7/27: NICU, awaiting surgery
- 7/28: surgery
- 7/28 – 7/31: CICU, recovering from surgery
- 8/1 – 8/05: Cardiac intermediate care, continuing to recover and regain weight
- 8/05: discharged!
I’ll go a bit into each of these stages, but the TLDR is that the days immediately following surgery, where she still had her breathing tube in, were the hardest for me.
1: Labor & Delivery
The only deviation a TGA baby will impose on labor is an increased odds of induction, as hospitals like to know when the baby will be born so they can plan for the surgery. My induction was scheduled for a week before my due date–though, as I was frequently assured, I was perfectly welcome to have the baby anytime after 37 weeks. I relayed this message to the baby, staring fondly and pointedly at the July 14th page of my planner, though a history of deliveries at 39 + weeks suggested this would be of little use.
As anticipated, I was induced. It is nice to know your baby’s birthday ahead of time, even if the physical process of induction has little else to recommend about it.
The lead up to delivery is where things started to really diverge from my prior birth experiences. The main divergence being that rather than a nurse and my obgyn and the odd medical student who happened to be hanging around the hallway at the right time, there was a small concert hall’s worth of people in the delivery room. Most of them were there purely for the baby, and lingered at the back of the room by the warming table until push came to shove, but still: I was very glad that this was my third baby, who came out in minutes, and not my second, who took two hours.
I’d been told that the baby would likely come out looking like any old newborn, and, if so, I’d be allowed 60 seconds of skin to skin. I spent most of it trying to see what color her skin was under all that gunk. I noted, too, that her eyes were open and she was crying, albeit in a slightly muffled sort of way. Certainly, I decided, she was alive. And then she was whisked to the back of the room. Pretty shortly thereafter, she was given some extra oxygen via a tiny CPAP mask, and for a moment, there was a possibility of her being put on a breathing tube, but her levels improved and she was sent off to the NICU. By the time I went up to see her, perhaps two hours later, she didn’t need the CPAP. IVs in each wrist administered prostoglandin, a medicine that keeps the PDA open, and a little bit of glucose. The nurse had sheathed her wrist in padded white sleeves, like a boxing gloves. Periodically someone would come by — her cardiologist, various neonatal pediatricians, lactation, social work. I would introduce myself to each new face and forget their names instantly, along with their roles and the folders of paper they handed me. Most of the time, though, it was quiet. I was able to hold our daughter straight away, and to feed her, and to marvel over her lilliputian perfection, just as I had with my sons.

2: Pre-surgery
We’d assumed that the surgery would be scheduled right after birth, and that this appointment would be one of those irrevocable ones, like a court date or the first date of school. Our daughter was born on a Wednesday; it was not scheduled at all until the following Monday, when we were told it would be Tuesday afternoon. On Monday evening, it was rescheduled to Wednesday morning. I don’t know if this is common to any hospital that offers pediatric cardiac surgery, or if it is common with pediatric surgery in general; our hospital was particularly busy with cardiac patients during this time, but they are often busy, and our daughter’s team seemed unphased by what seemed to us like a rather long time to go without a concrete date. Then again, her surgery was classified as elective, not in the sense that it truly was elective, but in that it wasn’t an emergency. She was, on account of her ASD and VSD, doing well enough that she could have gone another week, her surgeon told us — before quickly assuring us that it would happen Wednesday (Thursday at the very latest (but almost definitely Wednesday)).
There was a very real upside to this limbo: our daughter had a week to develop, to become acquainted with the NICU version of the outside world, and with us, her parents. Most importantly, she learned to eat. Eating, or difficulty eating, is the main thing that keeps babies in the hospital post-op, and babies that go into the surgery having already learned this skill tend to retain it.

The upsides outweighed the downsides, which were the breathlessness that comes with waiting without a date and so much sitting in a narrow recliner, half or three-quarters in the way of the nurse, that I thought my hamstrings might wither away entirely. When I wasn’t sitting in the recliner, I was sitting in a leatherette club chair in the lactation room, pumping and making my way through the audiobook of City on Fire. Or I was walking around and around and around the Longwood neighborhood and the Emerald Necklace and a very pretty part of Brookline full of fine old gothic revival Victorians while my husband sat in the recliner.
There isn’t room for two people to sit in a NICU bay — there really isn’t even room for one person to sit, if that person is in a recliner. In the NICU, I mostly read — Trust Exercise and Fundamentals of Play and Life Among the Savages and the August issue of Vogue and two New Yorkers and half an Economist and a smidge of Middlemarch and the aforementioned City on Fire audiobook and countless articles on my phone. Sometimes, I wrote in my notebook. Very rarely, I did some of the paperwork associated with having a child. I also did a LOT of what could charitably be called overhearing (less charitably: eavesdropping). There were four beds in our bay, and some of the nurses were chatty, either with the parents or among themselves. Over the course of a week, I got pretty invested in the other three babies — who wouldn’t? I also picked up a little of the nurses’ gerund-heavy shorthand: stating, drifting, rounding. And, I got an education in my daughter’s vital stats and the monitors that tracked them: the goals and the actuals, the beeps that were a result of squirming or cold feet or too many loops in the cord and the beeps that warranted a closer look (fortunately, our daughter didn’t have many of these).
The vital stats for a TGA baby are:
- Oxygen saturation
- Heart rate
- Blood pressure
- Breaths per minute
That was another way I passed time — nearly mindless, hypnotic time: gazing at the linear representations of my daughter’s life. The breaths per minute was the most erratic, regularly swinging from the high 80s to the low 20s. The oxygen saturation was the one I paid most attention to. The prettiest, by far, was the heart rate, with its long ventricular verticals and shorter atrial waves.

A note on noise levels: The NICU is not quiet, per se (though it can be hushed at night), but it’s not chaotically loud, either. Some babies cried, but not ceaselessly. The adults — the nurses and doctors and parents — uniformly used bedside voices. A friend remarked to me that her husband hadn’t been able to handle all the alarms, but I didn’t mind them — they sounded more like bells than beeps, unless the stats were well above or below goal, when they’d become very insistent.
3: Surgery
Our daughter’s surgeon told us that we should think of her open heart surgery like flying from Boston to New York: the actual flight itself is short, but it takes most of the day to get there. Boston to Atlanta would be a better analogy: two hours to get to the airport, checkin, get to your gate etc (getting all the lines in and the anesthesia and other meds going), three hours in air (going on bypass, the surgery itself, going off bypas), and another hour and a half to two hours to deplane, leave the airport, and get to your final destination (the cleanup or dry-out). All told, you’re looking at about a 6-7 hour ordeal.
It IS an ordeal — and yet: it’s progress. Forward movement. Wild, that there are people who can operate on hearts the size of walnuts. (I almost wrote “gods.” I was heading into the hospital the night before surgery, at maybe nine or so, and saw our daughter’s surgeon walking out and I really did think, a la Anthony Lane on the Armie Hammer character in Call Me by Your Name, “my god, he is a god.”) (I also thought: “hurry home and get some sleep!”)
The surgery was scheduled for 8:30 in the morning; the last time she would get to eat would be around 2 or 3. I’m mentioning this because I had a heart time with it — it may have been a genuine locus for my anxiety, or, in part, a proxy. But she was accustomed to eating every 2-3 hours, and I was sure she’d be ravenous by 8:30. Even now, it pains me to think of her waking at 5 or 6 and having no recourse for her hunger. But when we came in that morning, around 7:30, she was placid enough, wide awake and sucking gamely on her pacifier.

We each held her for a little while (and I worried again that she would start to root in my arms and I would be unable to stop myself from feeding her, and fuck up the entire surgery schedule, but this did not happen). The surgical team came up to go over the plan and we carried her down to the OR with them, a somber processional with a wedding train of tubes. “She’ll be asleep in a few minutes,” the anesthesiologist told me. The procession decoupled; Ottelie and her team vanished behind a double door, and a nurse took my husband and me across the floor, to the nurse liaison, a brisk, kindly older woman who acknowledged my tears without making a fuss over them, and gave us a list of the times she would call us with updates, and what each update would consist of. We were to expect calls about every 90 minutes, letting us know that 1) the lines had been placed, 2) she was on bypass, 3) she was off bypass, 4) they were finishing up, 5) the surgeon would be coming out to give us the final readout. Maybe there was one more call; already, I can’t remember.
We left the hospital. I went for a walk, and wrote up the birth story. Together, we watched White Lotus and and browsed the fiction stacks at Trident and picked up a lunch which we then redistributed to the neighorhood starlings. The calls proceeded more or less when the nurse liaison had said they would. The time between the second and third call was the most fraught, because, well: bypass. There was a chance — there is always a chance — that, when it came time to restart her heart, it wouldn’t, or not properly. I didn’t really think that would happen but even so. It is not an easy thing to know your child is on a heart and lung machine.
She came off the machine. She was “drying out.” It was time for us to return to the hospital. The surgeon came into the little waiting room, looking like a cat who’d swallowed a none-too-challenging canary. The surgery had gone perfectly, he said.
4: Post-Surgery

The cardiac team had prepared us for what our daughter would look like post-op. First, there would be an abundance of wires and tubes:
- Breathing tube
- Fluid tube
- Two chest drains
- arterial line for medications
- Two peripheral IVs
- Foley catheter
- Three pacing wires
- EEGs to monitor brain activity
- Heart monitors
Second, she would be puffy, especially around the eyes.
I prepared myself further by looking at the transpositionofthegreatarteries hashtag on instagram (and by paging ahead to see what the children looked like now, which was, for the most part, HIGHLY encouraging).
She didn’t look that bad, under all that spaghetti. She looked worse once the EEGs were added, a dozen little wire monitors stuck onto her head. She got puffier before she got less puffy (or “diaresed,” in medspeak). That first evening, we just looked down at her in her little isolette, and laid tentative fingers on a clear patch of forearm. The next morning, I attempted to draw what she looked like, because I didn’t want a photograph.
The breathing tube, though. When she was sedated (“snowed out,” in medspeak), it was okay, but once she woke up, there were times that I could tell it alarmed her. Her alarm coupled with its preventing me from feeding her engendered in me an intense animosity. (That ventilators, and what it means to go on one, have been such a weighty presence throughout the pandemic did not help matters.) I wanted it gone.
It was in for about a day and a half before the respiratory team deemed her ready to do a breath test (this is when they turn off the mechanical ventilation but keep the tube in, to see how the body breathes on its own). She passed, was extubated, and my peace of mind returned. I could no longer feed her on my own — a nurse needed to help position the chest drains and the foley catheter bag. But I didn’t mind, and those were all out by the following morning. The morning after that, so was she.
5: Intermediate Care + Discharge
The final part of her hospital stay was spent in a step-down room, which is like the standard room you go to after you give birth, only with more monitors and a crib instead of the adult-size patient bed. One parent is still supposed to sleep bedside, in a hideously uncomfortable cot, but I only did so for the one night required. The primary focus shifted to weight gain. This was initially fitful, as her diaretics were dialed up and down, but after a few days, she began to gain steadily. Her pacing wires were removed, along with her chest tube sutures. We were given lessons in drawing up and giving medication, in CPR, in (despite my mild protestations) breastfeeding. Our daughter was subjected to a 90 minute carseat test (despite her not-so-mild protestations). And then we came home. Today, she is four weeks exactly. As I write this, she curled on my stomach, hands (unsheathed) by her face. I keep thinking she’ll cant to the left or right, but she stays put.

End note
It is odd, isn’t it, that we still associate love with the heart? The heart is emotionless; it is entirely mechanical. It is the brain that dictates love, and the brain has nothing to do with the heart. We cannot live without the functions of the heart, but those functions can be replicated with literal pumps and tubes. There is no heart and lung equivalent for the brain. What I’m saying, I think, is that my daughter has a steampunk heart, and what of it? Her inside identifies, but it won’t define. That’s not defiance; it’s what I know to be true.
1. This won’t morph into a polemic against the way medical research papers are written — they are, of course, not written for me (often, it seems, they aren’t written for anyone at all). That said, their findings do make their way into laymen news media, and the frequency with which these are misconstrued or exaggerated suggests a little clarity of language, a gesture towards interpretability, might go a long way.
2. They mostly died while these procedures were being developed, too. This piece goes into the history of the Mustard/Senning procedures with slightly more stylistic flair than your average medical journal; for all that, patient deaths, which were very frequent in the initial years of development, are recounted with dry numerics. I suppose death doesn’t need descriptors, but it’s a wonder the surgeons kept going.

Leave a comment